After the war–Vietnamese dementia caregivers repay a lifetime of love

By Christine Nguyen
Two evacuations It was August 24, 2017, one day before Hurricane Harvey hit Houston and dumped more water than any storm ever recorded in United States history. In a few days, Houston saw as much rain as it usually saw in a year.
My brother picked up our dad, who was 82, at his house, where he lived alone, and they evacuated to higher ground. They rode out the storm in the countryside. My brother’s in-laws had gotten 10 pounds of ground beef and made enough chili to last through the storm. This is Texas, ya’ll.
My brother said Dad seemed confused after he was evacuated to someone else’s home. Dad crapped on the floor, and at night he paced in the spare room, yelling to himself. My brother listened through the wall, just like when we were kids. I was embarrassed that my sister-in-law had to witness Dad’s erratic behavior. Dad picked at the plates they made for him. He didn’t eat any chili. With my brother’s help, I called him on FaceTime. He looked terrible. His hearing was bad, and he refused hearing aids, so as usual, we couldn’t have a real conversation. I felt helpless, but at least he was safe.
Then a week after he fled Houston, Dad convinced my brother to take him back to his house. He would be fine, he insisted. He had a case of Ensure Plus. This news rang some alarm bells, but I crossed my fingers. Dad had survived worse.
But a few days later, when my brother came to check on him, Dad didn’t answer the door. TV news was blaring. Inside, Dad was on the couch on top of some towels, incontinent and barely responsive. My brother brought him to the emergency room, and Dad got admitted to the intensive care unit. He was 86 pounds.
My brother called me for advice and reassurance. What was going on? I'd had a sinking feeling about Dad for a long time. But even though I'm a doctor, I hadn't been able to face the truth until his hospitalization — Dad had dementia.
I sent my brother information from the Alzheimer’s Association about signs of dementia, many which described Dad. His sudden deterioration during the hurricane wasn’t just stubbornness or being a stereotypical grumpy old man. When someone has dementia, a change from routine can make them worse. Experts call it transfer trauma. Maybe the evacuation from Hurricane Harvey reminded him of that last day of April 1975. That month marked the end of the Vietnam War, when the communist North triumphantly rolled tanks through Saigon, the capital of the defeated South. Families climbed over each other to evacuate on US airlifts. But Dad had been in the South Vietamese army, and he believed in defending his country to the end. He refused our family’s spot on an American C-131 aircraft. For more than 40 years, he had continually relived the decision.
Unlike Dad’s decision to stay, refusing to leave a sinking ship, my family had chosen a different path when Hurricane Harvey pounded the Texas coast. We thought that evacuating Dad from the storm would make him safer. And from a purely physical perspective, he was. But the transfer trauma from the move increased his overall chance of dying by three times. To this day, my family doesn’t really discuss Dad’s dementia. Although dementia is the top diagnosis in older adults, most families and doctors don’t recognize it. Furthermore, Asians like my family have a higher incidence of vascular dementia than the general population.The research specifically into Southeast Asians is sparse. They have many risk factors for dementia.
Cultural expectations of normal
It’s hard to find other Vietamese willing to talk about their family members with dementia. But Quyên Vương is an outspoken community leader. She and her father live in Santa Clara, California.
We speak under the gaze of several large stone and gilt Buddhas that protect her home. Quyên lays a chux, one of those absorbent blue hospital pads, on a dining chair for her father to sit on. Her father’s given name is Quả, but when he became a U.S. citizen, he changed his name to Bob, after Bob Hope, the comedian that entertained US troops during the Vietnam War. Taking the name of a famous American entertainer was an expression of his love for his new country.
As Quyên speaks, her father holds a necklace of beads. Every day, he chants “Nam mô A Di Đà Phật,” the homage to the Amitabha Buddha. After each recitation, Bob counts off a number. Quyên compares his repetitive chanting to some of his other behavior at home.
“There’s a lot of repeating. It’s like a broken record. It goes back to that groove and it plays that part.”
When I ask Bob different questions, he often answers with the same story of his childhood — losing his father at 11 and begging relatives for support for his mother and younger siblings. He laughs with a deep sonorous voice.
“He gets emotional and laughs but sometimes it looks like he’s crying,” Quyên says to explain Bob’s incongruous affect when he speaks.
A few years ago, when Bob got more and more combative, Quyên chalked up his erratic behavior to his personality and his position as the family patriarch. “I didn’t know dementia was coming on, I thought it was him just being him himself. His usual self — very demanding, very authoritative.”
Cultural expectations made Quyên interpret his behavior as normal. In her memory, he had always snapped at people. Her father had grown up with the advantage of being the oldest male child in a traditional Vietnamese family. She saw his imperious behavior as just another expression of his privilege.
“He was trying to get things his way. The way he has always been doing all these years.”
When she went on doctor’s visits with him and brought up his aggression Quyên didn’t get much information.
“The doctor never officially called it dementia. She just said, ‘Yeah, old age, he probably has dementia.’ To me there was no official diagnosis, so we just assumed and kind of thought of dementia as old age, senility.”
To Quyên and her family, senility meant his behavior was an inevitable product of aging. But the truth is, dementia is not normal aging. There are a number of diseases and health conditions that bring on dementia. After Alzheimer’s disease, strokes are the second most common cause. Bob had had a stroke, but his doctor never spelled out the connection.
Struggling for diagnosis
Oanh Meyer is an Assistant Professor in the Department of Neurology at the University of California at Davis. She studies cognitive and mental health disparities in racial and ethnic minorities. Meyer explains that unlike genetic risk factors, which people can’t change, there are factors people can modify, such as smoking, high blood pressure, obesity, and diabetes. Social factors such as poverty, education level, isolation, and depression also play a role in how likely a person is to develop dementia. Unfortunately, those issues, and how to address them, aren’t always addressed in primary care. Meyer shared her family’s own experience trying to get a diagnosis as well as guidance from her mother’s doctor.
“He took her blood pressure every time she went in and that was pretty much about it.”
The doctor shrugged off her mother’s memory problems. “Oh, she’s fine,” she remembers the doctor saying.
As a researcher in health disparities, Meyer knew she had to push for her mom to see a neurologist. When they did see a neurologist, that specialist prescribed medicine but didn’t explain what the family should expect. When Meyer told her mom she needed to ask her doctor more about her symptoms, her mom pushed back.
“There was concern on her part about offending her doctor. Or not wanting to hurt his feelings or question his authority.”
Risk factors for developing dementia
Asking questions is important because knowing the answers can help patients and families modify the risk factors they can control. For instance, with my dad, there were plenty of things that put him at risk for dementia. Like a lot of Vietnamese men, he had been a smoker. Despite being athletic and thin, he still had high blood pressure and heart disease, both strong risk factors for dementia. A 2019 study from the American Heart Association shows Asian Americans die sooner from heart disease and stroke than whites. Among Asians, Vietnamese are one of the two subgroups who suffer the most from strokes.
For years to save money, Dad took only half his heart medications. He rarely went further than the mailbox, and even then, he got out of breath. Indoors, he cranked up the TV and watched sports, drawing the drapes and turning off the lights to shut out Houston’s brutal summer. Air conditioning was too expensive to use. Like a lot of older people living alone, he was isolated.
Taking a look at how dad deteriorated after the hurricane evacuation, I wondered about my father’s physical and psychological trauma from his years in the Vietnam War. Was this another risk factor for dementia? When American vets returned from Vietnam, many had paranoia and flashbacks. The Vietnam Vet experience defined PTSD, or post traumatic stress disorder. We now know vets with PTSD are more likely to develop dementia. But there hasn’t been much study of Vietnamese PTSD. The available research shows it's common among Vietnamese who went through the war.
Caregivers are hidden patients
When I talked to Oanh Meyer and others who study the Vietnamese community, it became clear that trauma from the long and brutal war, the repression of the new communist government, and the refugee experience all contributed to collective trauma. Vietnamese pride themselves on resilience and many have sublimated the trauma, but it remains a frequent visitor in memories. Quyên, who’s taking care of her father Bob, vividly remembers the peak of the war. The entire extended family of over 30 hid in her grandparents’ house as fires raged in different districts of Saigon.
“We were sleeping in the middle of the night and there would be shooting or bombing ... we would run so fast we would hide under the big bed and they stacked a lot of sandbags.”
She fled Vietnam on a boat when she was 16 as an ‘unaccompanied minor.’ Her father and older siblings had already left the country. She was in charge of escorting her little brother. Like in many traditional Vietnamese families, boys and men and older people had first priority.
Quyên was one of the lucky ones who survived the ocean trip. About 400,000 “boat people” died at sea. Yet at the peak of the refugee crisis, ⅔ of Americans didn’t want the Vietnamese in the U.S. One of the worries was they would suck up social services. A New York Times article at the time quoted some Americans who were worried about “Asian diseases” and drugs. In part to prove their worth, Vietnamese internalized the desire to be “good minorities.” Quyên’s dad rejected programs like welfare, fearing they would stigmatize him as a societal burden.
Officially, the Vietnam War lasted about 20 years. Over 3 million Vietnamese died. The anniversary of Black April, the day Saigon became Ho Chi Minh City, is a day of mourning for expatriates. Quyên’s father relives the end of his nation like it was yesterday.
“He talks all about the bad things that the communists did to him.”
If she tries to change the subject, it can set off a rage.
“He’s like ‘NO! You’re a communist! You’re a communist!’”
Quyên says dealing with the combination of trauma and dementia is hard for her father as well as herself.
“There’s still so much hatred, unhealed wounds from the war inside. There are days that he would wake up and he got really angry because of some news he heard on the radio the day before so he would be screaming and shouting: ‘On behalf of, representing GOD! I’m just gonna punish them!’ It’s so much negativity.”
Caregivers of people with dementia are “hidden patients.” According to Oanh Meyer, the researcher at UC Davis, the stress causes biological changes that make caregivers more prone to health problems and actually shortens their lifespans. Taking care of caregivers is important, she says, because research shows that caregivers’ physical and mental well-being affects how the patient fares.
Quyên points out how her caregiving responsibilities put a strain on relationships with other people.
“I’m risking my health and thank God I’m divorced ... because I don’t think any man would put up with taking care of a father-in-law like this.” It sounds like she’s making a joke, but she’s dead serious.
When Quyên first started taking care of her father, she quickly felt trapped. Taking care of her dad was a series of small daily battles.
“One day I was telling him that I smell something, so you need to change your diaper. And he said ‘NO! I am clean! I’m cleaner than you!’”
Daughterly duty became resentment. When her dad announced he wanted to live to a hundred, she answered, “Okay Daddy, you live to 100, I’m going to die early.”
Taking care of her father was one of the toughest challenges of her life, but she kept her problems to herself.
“It’s so hard to talk to the siblings. The cultural expectation is just so heavy. It just never seems enough.”
Wrenching choices
Quyên’s story is familiar to me. I go to Houston regularly to visit and care for my dad. I keep my expectations low, which is the best way to avoid frustration. First, do a sweep of his room, removing the three months of hoarded napkins and saltines stuffed in socks. Throw out wet diapers he’s hung up to reuse. He hates my organizing attempts. He says he’s got everything in its place. Dumping his stuff seems mean, but I don’t want him to trip and fall or get sick from rotten food.
I’ve been ashamed to admit my father is in a nursing home. It looks like the easy way out. After dad’s hospital stay, we knew he needed 24-hour care. He was too frail and combative to move on a plane, and I wasn’t sure my marriage would survive bringing my dad to my home. My brother’s young family lived in a narrow 3 story townhouse. How was Dad going to move around there? A nursing home seemed like the best choice.
For a while, he seemed to do better, but I know it’s not the choice I would have made if everything I wanted was possible. His nursing home posts a monthly activity calendar so you can picture the residents doing chair yoga or playing bingo. But mostly everyone just sits and waits. Dad usually sits in the dining room alone, waiting an hour to get his Salisbury steak and mashed potatoes. He started to stay in his room during meals.
“Food costs extra here,” he tells me.
It’s pointless explaining to him that it’s a package deal. After initially gaining some weight, he slid back down. When your dad, who is 5-foot-8, drops down to 86 pounds, healthy food isn’t even an issue. You want maximum calories. So when I visit, we go to his favorite fast food places — Jack in the Box, Popeye’s, and Burger King. Forget bingo, we buy lotto tickets. He’s an old pro. He’s still mad my brother lost what he believed to be a $4 million winning ticket. I like helping him play lotto because it makes him happy, and counting the numbers and figuring the odds seems like good mental exercise.
Dad insists on walking when he goes outside. But back inside the nursing home, he collapses into his wheelchair, whistling his breath through pursed lips. It’s hard for him to go back into the nursing home after a taste of freedom.
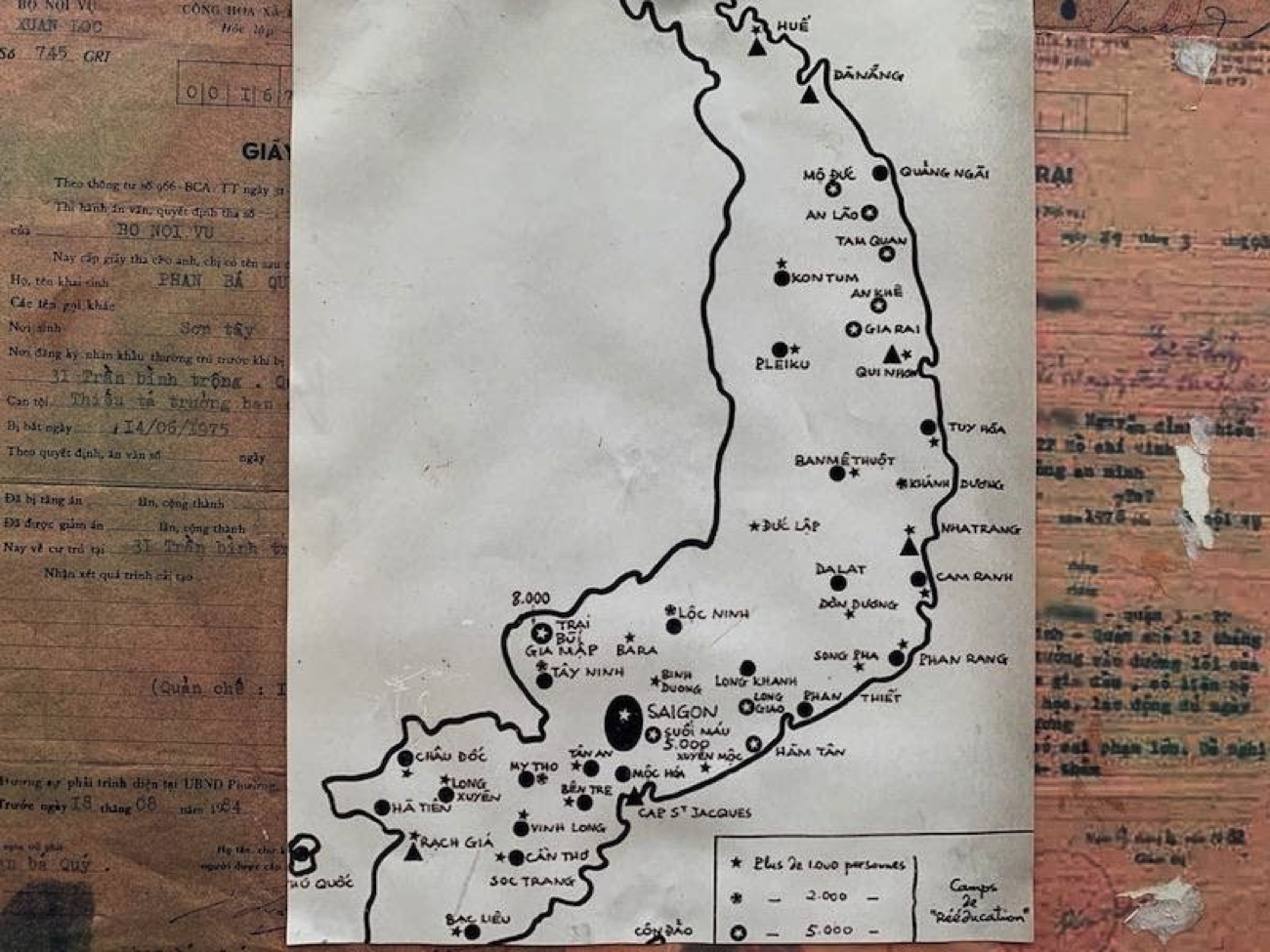
From 1975 to 1993, over 300,000 people were imprisoned in Vietnamese reeducation camps.
“I go and I’m very tired. Because normally I can’t get out of the building,” He says. “It’s like a jail, like a prison.”
These words are hard for me to hear. In 1978, the new Vietnamese government forced my family into a so-called “reeducation camp.” It was a prison. One day, my brother and I, our heads freshly shaved to control lice, went to Dad’s cell. He was packed in an 8-by-8-foot box with so many other men, they had to take turns lying down. Through the bars, we gave dad the banana we’d gotten as a prize.
On a recent visit to Houston, Dad asked me to drive by his house, the one he’d almost died alone in. I felt awkward going past it, like I had taken his home away from him. We’d had a long day — Popeye’s Fried Chicken and then LensCrafters. To finish, on the way back to the nursing home, I’d gotten him a frozen taro drink from 85C Bakery. I’m happy the chain’s best tasting drink packs a whopping 500 calories. His eyes flashed when the straw brought the purple shake to his lips. There was just a little drink left in the cupholder. Dad’s right eyelid doesn’t close completely — an old injury — so I wasn’t sure if he was asleep. Then he reached out to me and patted me on the arm. To acknowledge that he knew I had made an effort.
More research is needed
In my investigation into dementia caregiving for Vietnamese, I found only two researchers in California, where there’s the biggest population of Vietnamese in the U.S. Oanh Meyer’s colleague Vân Mỹ Tạ Park is an Associate Professor at University of California San Francisco and researches public health. She points out older Asians are projected to grow by 352% by 2030. They’re the fastest growing minority, but there’s not enough research or manpower.
“When you look at the national centers for Alzheimer’s disease across the country, probably a percent or less of the people are Asian Americans.”
When Asians are mentioned at all in research, they’re lumped into a single category that includes 30 different countries and over 100 different languages. It makes invisibility worse. There are over 2 million Vietnamese in the U.S. When you break it down, factors like health literacy, income, and the ability to speak English are different and affect access to care.
“We need to be at the table,” Park says. “If you don’t participate in research you can’t get the culturally tailored programs and treatments that you would want.”
Park explains what’s available at most doctor’s offices is a cut and paste approach.
“They would go to the Alzheimer’s Association website, which has materials in Vietnamese, and print them out. Unfortunately, that’s the standard of care.”
Like Meyer at UC Davis, Park at UCSF is focusing on improving dementia care through supporting caregivers. Park explains many Vietnamese caregivers, who grow up inculcated with the rules of filial piety, are reluctant to ask for help. Admitting the need for help is viewed as whining and a personal failing.
“If you frame it as ‘focus on your own mental health’ and ‘go get some respite care,’ it’s like, ‘what are you talking about?’”
Park is trying to find culturally acceptable ways to address, and eventually reduce stress and depression. One way she’s getting caregivers to open up is to use Korean dramas. Vietnamese caregivers can identify with the Asian faces and Asian themes of these K-Dramas, which are a worldwide streaming phenomenon. In one intervention, Park’s research participants were grouped together to watch a K-drama. The TV episode showed a doctor struggling with dementia symptoms, agreeing to get help only if her problem is kept a secret. After watching the drama, Park’s research participants were able to open up.
“They were very talkative. They could relate and they could understand. Everyone talked about the stigma and the shame as it relates to knowing.” The research participants became their own support group. This is unusual because Vietnamese don’t usually go to support groups or participate in research. Park explains that Vietnamese caregiver’s reluctance to participate in research and support groups stems from past experience with government surveillance and repression.
She says questions that she gets include,‘How would this look if I participate?,’ ‘What information are you getting from me?’ and ‘What are you going to do with this information?’
Park is trying to overcome the data gap. In 2019, she received a National Institutes of Health grant to fund over $3 million in research in four different sites in California. She plans to recruit 10 thousand participants.
In 2018, Park presented earlier research to Vietnamese in San Jose. Over 100 people came. Quyên Vương, who started out as a study participant, became the facilitator for the entire meeting. She says opening up about her struggles and participating in Park’s research program have helped her.
“Once I stopped feeling guilty, I stopped the resentment.”
She has been able to turn to a regular Vietnamese women’s support group as well as her faith in Buddhism. Her faith has given her some comfort.
“It helps me to practice compassion. But it also helps me to understand more about karma. If one day I have to send him to a nursing home, that’s his karma, nothing I can do about that, because it is his karma, and I’ve done all I could.”
Karma. For now, my own father is still in a nursing home, despite my misgivings. On a recent trip, on our last night in Houston, my kids and I brought Dad pizza. When I stepped away, my older daughter recorded her grandpa. The recording was the most lucid conversation I’d heard in a long time. He told her how special I was. I was sad to have missed it, but was glad my kids saw a different side to him. Before we left, I reminded him to keep eating – “Bố nhớ ăn nhé.” Remember to eat, Daddy.
This story was made as part of a fellowship from the Gerontological Society of America, Journalists Network on Generations, and the Silver Century Foundation.